London Bridge has fallen down

Eighteen days out, and I figure it’s time to explain what’s actually going to happen on June 30. Not “foot surgery.” The real thing, all five jobs, one anesthesia bill.
The easiest way to understand it is to picture a suspension bridge.
Your arch isn’t a solid structure. It’s a span held up under tension. The main cable doing that work is the posterior tibial tendon, which runs down the inside of your ankle and pulls the arch up with every step. Underneath, a ligament called the spring ligament acts as the bridge deck: a hammock of tissue the arch actually rests on.
My main cable frayed. And when the cable goes, everything downstream goes with it. The deck stretches out, the foundations drift out of alignment, and the whole span starts to sag. That’s why my foot didn’t just hurt. It visibly collapsed: heel tipping outward, arch flattening toward the floor. London Bridge, fallen down.
(Yes, fine, the pedants are correct: London Bridge is not a suspension bridge. The nursery rhyme just has better name recognition than my ankle. If you want anatomical accuracy, picture the Union Chain Bridge instead. That’s it in the photo up top: opened in 1820, the oldest suspension bridge in the world still carrying traffic. Two hundred years of cables under tension and still holding its span. Now that is a recovery goal.)
You can’t fix a failing bridge by tightening one bolt. So here’s the actual work order, keyed to the diagram.
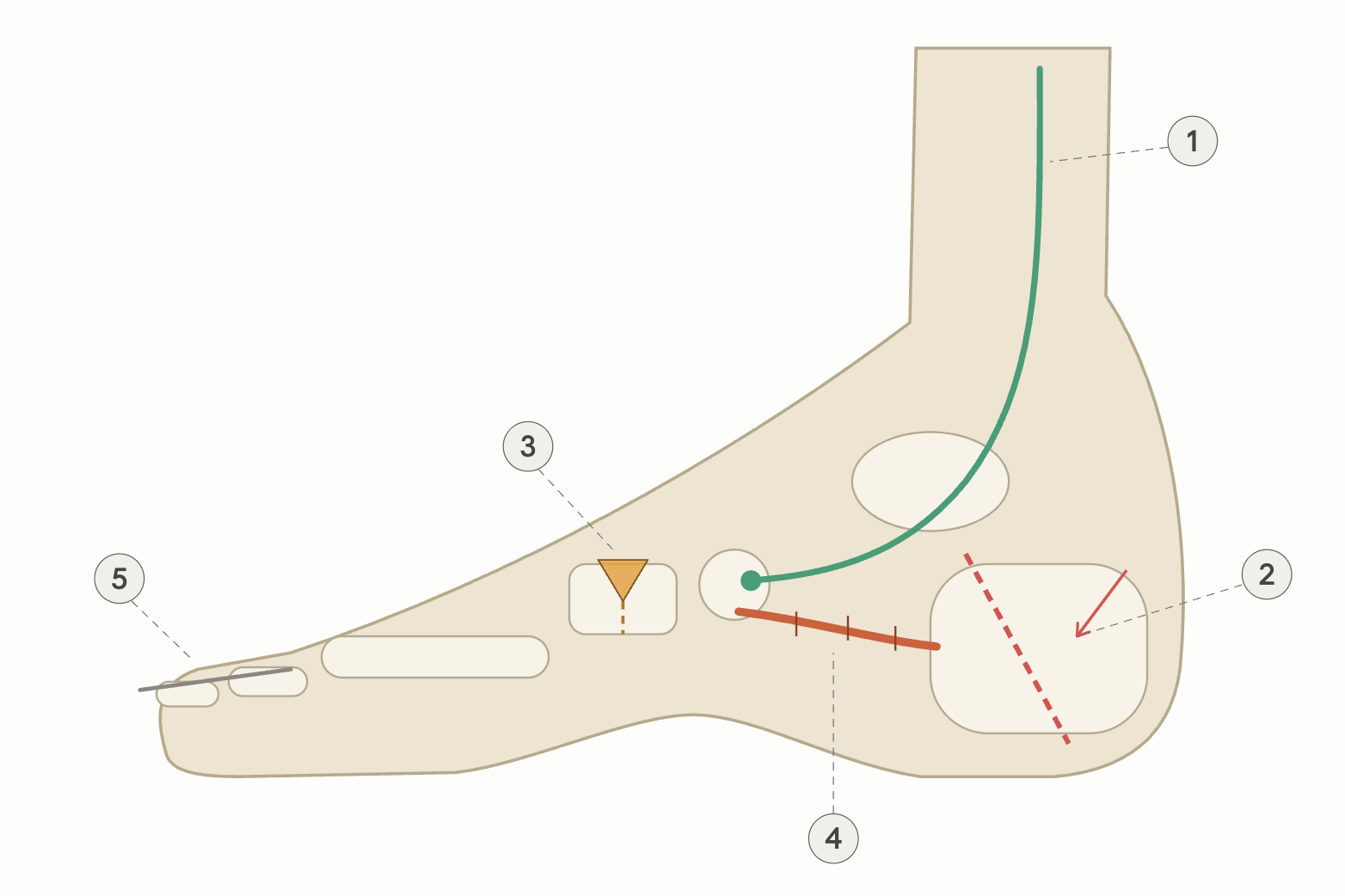
1. Replace the main cable (the teal line): FDL tendon transfer. The worn-out posterior tibial tendon doesn’t get patched. It gets a replacement. The surgeon borrows a neighboring tendon, the flexor digitorum longus, which normally curls my smaller toes, detaches it, and anchors it into the navicular bone at the top of the arch. From now on, its full-time job is holding the arch up. And no, I won’t miss it. The foot ships with enough redundancy in its toe-flexing muscles that other ones cover the curling, and most people never notice the difference. Genuine biological spare-parts engineering.
2. Re-seat the foundation (the red dashed line): heel cut and shift. Osteotomy number one. The calcaneus, my heel bone, gets cut clean through, and the back piece slides inward toward my midline by several millimeters, then gets fixed in place with a screw or two. This re-aligns the heel under my leg so the Achilles pulls straight instead of pulling the foot further into collapse.
3. Shim the span (the amber wedge): midfoot wedge. Osteotomy number two. A small wedge is opened into a bone in the midfoot, which tips the big-toe side of my foot back down so the front of the foot meets the ground the way it’s supposed to. When a bridge settles crooked, you shim it level.
4. Re-stitch the deck (the stitched orange line): spring ligament repair. That hammock the arch rests on stretched out when the cable failed. The surgeon stitches it back tight, sometimes reinforced with suture tape, so all the bone work above it doesn’t sag back over time.
5. One more while we’re in there (the gray wire): hammertoe repair. Different problem, same trip. The bent middle joint of my second toe gets straightened, usually by removing a sliver of bone at the joint and holding everything in line with a temporary wire. The wire sticks out the tip of the toe for a few weeks and then gets pulled in clinic. It’s exactly as weird as it sounds. Yeah, I’m a little freaked out about that one, too.
Why five procedures instead of one? Because soft tissue alone stretches back out, and bone work alone leaves nothing actively holding the arch up. The whole bridge gets rebuilt, or none of it holds.
Turns out the nursery rhyme had the engineering right all along. When the bridge falls down, wood and clay wash away, bricks and mortar will not stay. You build it up with iron and steel. In my case: titanium screws, suture tape, and one borrowed cable.
- I can finally explain my own surgery without hand-waving
- Which midfoot cut am I getting: a Cotton (wedge into the cuneiform) or an Evans (lengthening the outer edge of the heel)?